

- Home
- Volume 26 (2022)
- Numéro 2
- Quantitative and comparative analysis of ethnomedicinal plants from the Lasdana (Azad Jammu and Kashmir)


View(s): 3565 (25 ULiège)
Download(s): 907 (7 ULiège)

Quantitative and comparative analysis of ethnomedicinal plants from the Lasdana (Azad Jammu and Kashmir)

Résumé
Analyse quantitative et comparative de plantes ethnomédicinales de Lasdana (Azad Jammu et Cachemire)
Description du sujet. L'ethnopharmacologie est importante car elle aide à une bonne connaissance des interrelations de nombreux aspects, ainsi que de toute la culture pratique et intellectuelle des personnes avec des plantes.
Objectifs. L'objectif de cette recherche est de documenter et de comparer les connaissances traditionnelles sur la diversité des plantes médicinales à Lasdana, district de Bagh Azad, Jammu et Cachemire.
Méthode. Les informateurs ont apporté des connaissances ethnopharmacologiques par le biais d'entretiens et de discussions de groupe, qui ont été examinées à l'aide de plusieurs paramètres quantitatifs.
Résultats. Cent-quarante espèces de plantes médicinales ont été identifiées, réparties en 123 genres et 54 familles. La famille des astéracées était la plus courante (14 espèces) et les herbes étaient les plus courantes (contribution de 72,85 %), les feuilles étant l'élément végétal le plus couramment utilisé (74 espèces). La façon la plus courante de produire un remède était d'en faire une décoction (45 espèces végétales). Les maladies circulatoires avaient le score le plus élevé du facteur de consensus de l'informateur (ICF) (0,92). La fréquence relative de citation la plus élevée a été trouvée dans Thymus linearis Benth. (0,89), Geranium wallichianum D.Don ex Sweet (0,89) et Berberis lycium Royle (0,88).
Conclusions. Des recherches pharmacologiques et pharmaceutiques sur les espèces végétales thérapeutiques vitales devraient être menées pour appliquer en toute sécurité les connaissances traditionnelles à une population plus large.
Abstract
Description of the subject. Ethnopharmacology is important because it aids in a proper knowledge of the interrelationships of many aspects, as well as the entire practical and intellectual culture of people with plants.
Objectives. The objective of this research is to document and compare traditional knowledge about medicinal plant diversity in Lasdana, District Bagh Azad, Jammu & Kashmir.
Method. Informants contributed to ethnopharmacological knowledge through interviews and group discussions, which was examined using multiple quantitative metrics.
Results. There were 140 medicinal plant species identified, divided into 123 genera and 54 families. The Asteraceae family was the most common (14 species), and herbs were the most common (72.85% contribution), with leaves being the most commonly used plant element (74 species). The most common way to produce a remedy was to make a decoction (45 plant species). Circulatory diseases had the highest informant consensus factor (ICF) score (0.92). The highest relative frequency of citation was found in Thymus linearis Benth. (0.89), Geranium wallichianum D.Don ex Sweet (0.89), and Berberis lycium Royle (0.88).
Conclusions. Pharmacological and pharmaceutical investigations on vital therapeutic plant species should be done to safely apply traditional knowledge to a larger population.
Table of content
Received 14 July 2021, accepted 28 March 2022, available online 5 May 2022
This article is distributed under the terms and conditions of the CC-BY License (http://creativecommons.org/licenses/by/4.0)
1. Introduction
1The study of ethnobotany is of great importance for the aid it gives to a proper understanding of the interrelations of all the several traits and of the whole material and intellectual culture of a people in its entirety. Medicinal plants have been used in traditional healing practices since ancient times. This natural resource has been exploited in different ways by indigenous communities (Adnan et al., 2014). Many local communities in developing countries are still dependent upon herbal medicine as a less expensive, easily available, and holistic, often culturally based, resource for primary healthcare (Srithi et al., 2009; Aziz et al., 2018). According to the World Health Organization (WHO), 80% of the world population use medicinal plants for treating ailments (Shinwari, 2010).
2The knowledge on medicinal plants is mostly transferred orally from older to younger generations and in this way preserved among many indigenous communities across the globe (Pieroni & Quave, 2005; Bano et al., 2014a). However, this knowledge is gradually decreasing with rapid urbanization and wider availability of modern health systems (Ladio et al., 2007; Vitalini et al., 2013; Baydoun et al., 2015). This decline makes ethnobotanical and ethnopharmacological surveys of paramount importance (Verpoorte et al., 2005; Heinrich, 2008; Bibi et al., 2014).
3Pakistan is a floristically wealthy country harboring about 6,000 species of higher plants. Of these species, more than 12% are used medicinally, and active constituents of about 500 plant species have been reported (Shinwari, 2010). Due to its unique geographical location and diverse habitat, Azad Jammu Kashmir (AJK) carries a rich and diverse medicinal flora with wide indigenous usage among the rural communities.
4While a variety of studies has compiled ethno-medicinal information of plants in various parts of Pakistan, including Azad Kashmir, the mountainous area of Lasdana has never been assessed ethno-botanically due to its remote location and hilly terrain, along with religious and cultural restrictions (Amjad et al., 2017). In our study, we hypothesized that socioeconomic aspects would impact the distribution of traditional knowledge and that furthermore the usage or importance of plant species may vary among the local communities although having the same culture.
5Therefore, the current study was designed to explore and investigate traditional knowledge of medicinal plants utilized for health issues. The data was quantitatively analyzed and compared with previous reports to determine the novelty of the work.
2. Materials and methods
2.1. Study area
6Lasdana is a mountainous region that lies between 73°56’E to 73°58’E longitude and 33°55’N to 33°57’N latitude. The altitude of area ranges from 1,785-2,750 m. The collection sites in the study area are presented in figure 1. The area is a visitor resort and is especially popular among tourists owing to its weather and natural beauty. The climate is of temperate type.
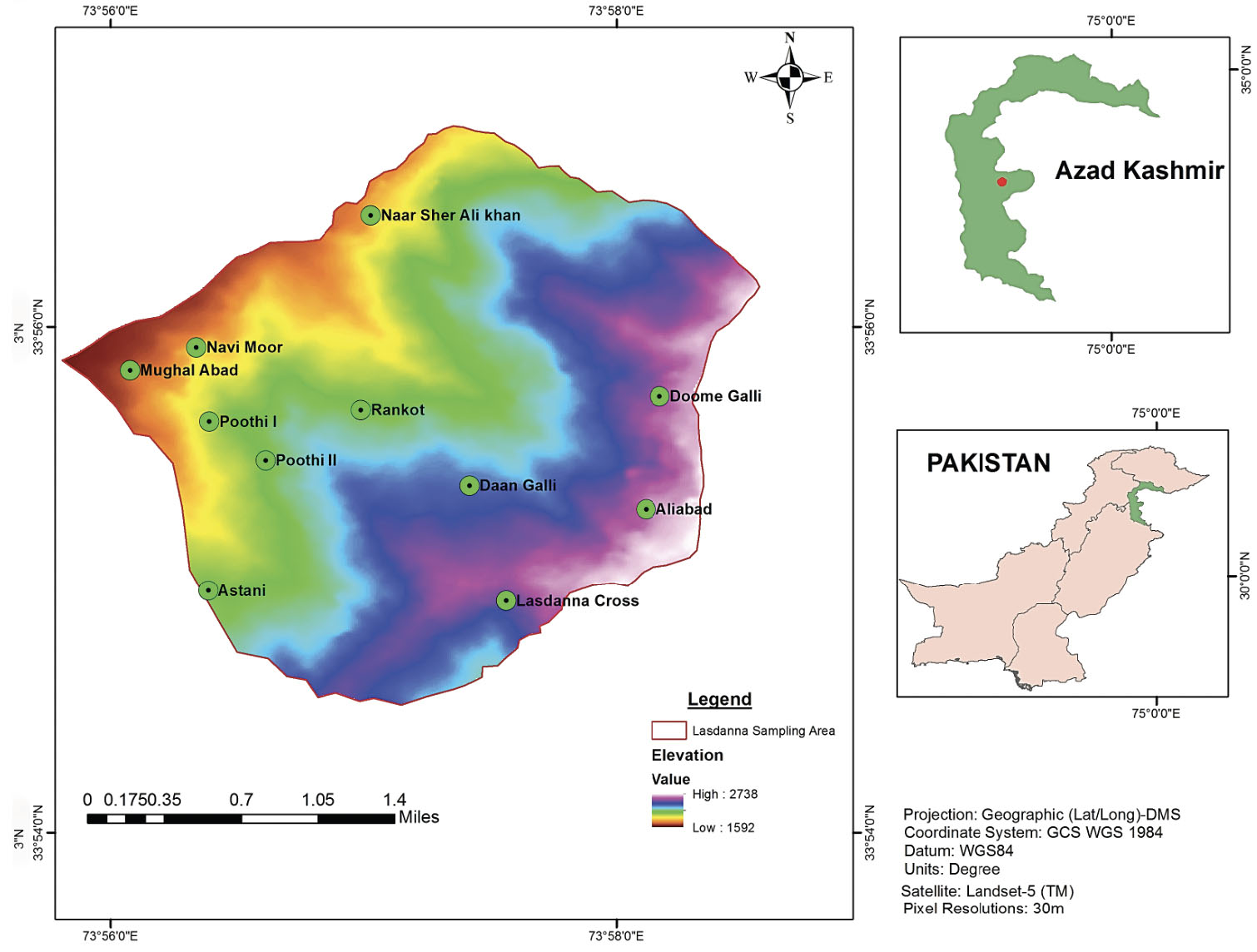 Figure 1. Map of the study area — Carte de la zone d’étude.
Figure 1. Map of the study area — Carte de la zone d’étude.
7The average annual temperature in Lasdana is 10.7 °C. July is the warmest month throughout the year with an average 19.4 °C temperature around the year. The lowest average temperature is recorded during January, when it is around -0.8 °C. The average annual precipitation is 1,554 mm. Precipitation is maximum during the month of July (212 mm) and minimum during the month of October (45 mm) (Figure 2). The data was provided by the meteorological department upon request.
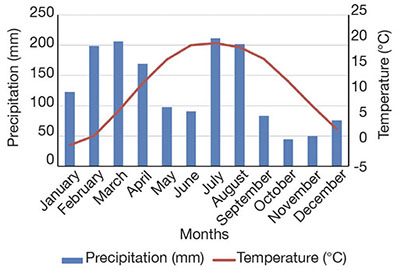
Figure 2. Precipitation and temperature of the study area — Précipitations et température de la zone d’étude.
8Most of the inhabitants of the region are nomads. They spend the summer at higher altitudinal areas of the national park along with their livestock. Before the arrival of winter, they shift the livestock to the plain areas. People are mostly dependent upon summer tourism for their livelihood. Most of them are tour guides, rest house managers, restaurant workers, shop keepers and jeep drivers. Some were part-time or full-time shepherds and farmers.
2.2. Collection and identification of specimens
9Field surveys were conducted during different seasons from July, 2017 to June, 2018. Specimens of each plant species were collected from different localities in triplicate. They were carefully pressed, dried and properly mounted on herbarium sheets. The collected plant specimens were identified using the Flora of Pakistan (https//:www.eflora.com) (Nasir & Ali, 1972; Nasir & Ali, 2010). APG IV 2016 was used for the correct family name (Chase et al., 2016) while ‘Plants of the World online’ was followed to find correct scientific names (The Plant List, 2013). Identified specimens were cross checked with vouchers in the AJK medicinal and aromatic plant herbarium of PARC (Pakistan Agricultural Research Council). The voucher specimens were deposited at the herbarium of Women University of AJK, district Bagh.
2.3. Ethnopharmacological data collection
10A total of 68 participants of different ages (19-75 years) were interviewed by using semi-structured and open-ended questionnaire to collect ethnomedicinal information. Participants were selected randomly from different age groups to get maximum information. In addition, group discussions and field observations were conducted (Bruni et al., 1997; Heinrich et al., 2009; Ghorbani et al., 2011). The questionnaire was developed following Edward et al. (2005). The informants were selected randomly, and the sample size was chosen by using method of Kadam & Bhalerao (2010). The Code of Ethics of the International Society of Ethnobiology (http//:www.ethnobiology.net) was followed. Ethical approval for conducting survey was granted by the ethics approval committee of Women University of AJK, Bagh. Legal permission for interviews was granted by the municipality committee of the investigated area. Written prior informed consent was taken from the informants before acquiring information (S1).
2.4. Quantitative analysis
11Quantitative indices including Use Value (UV), Relative Frequency of Citation (RFC), Informant Consensus Factor (ICF), Relative Importance (RI), Jaccard Index (JI), and Fidelity Level (FL) were used to evaluate the significance of medicinal plant species.
12Use value (UV). Use value reflects the local significance of a medicinal plant in the area. It was calculated following Vijayakumar et al. (2015):

13with Ui, the number of uses for each species by number of informants; N, the total number of informants.
14Relative frequency of citation (RFC). RFC indicates the importance of each plant species based on frequency of citation. It was calculated following Vijayakumar et al. (2015):

15with FC, the number of respondents mentioning the use of a particular species and N, the total number of respondents.
16Informant consensus factor (ICF). The consistency between the informant and plant species used for curing particular group of ailments was tested by utilizing the ICF. It was calculated following Heinrich et al. (1998):
17where Nur is use-reports in each disease category and Nt, the total number of species reported by all informants for a particular category of disease. The value of IFC ranges between 0-1. A high value of ICF reflects plant species chosen based on well-defined selection criteria and information about the plant for curing particular diseases with a maximum coincidence among the informants. Whereas low ICF value shows that there is random selection of species and minimum exchange of information about plant species for curing particular disease categories among the community.
18Relative importance (RI). RI was calculated using the formula of Khan et al. (2015):
19where PH represents pharmacological property of each plant species and Rel PH represents the relative number of pharmacological properties attributed to a single plant.

20with BS, the number of body systems healed by an individual plant species and Rel BS is the relative number of body systems treated by individual plant species.
21Jaccard index (JI). The Jaccard index was applied to determine similarity of knowledge between different communities comparing uses reported in the current study with published ethnobotanical data in the region and at global level. It was calculated using Gonza et al. (2008):

22where a represents the total number of medicinal plant species of the study area; b is the total number of species reported in adjoining/comparing area; and c is the number of common plant species of both areas.
23Fidelity level (FL). The fidelity level is used to elucidate the most preferred species for curing a particular disease. The fidelity level was calculated following Alexiades & Sheldon (1996) using formula:
24where Np represents respondents’ number of use reports of a plant species for curing a specific disease and N is the number of total respondents reporting the respective plant species for any ailment. A high FL value of a species reflects a high frequency of use for particular ailment by local inhabitants.
3. Results
3.1. Demographic data
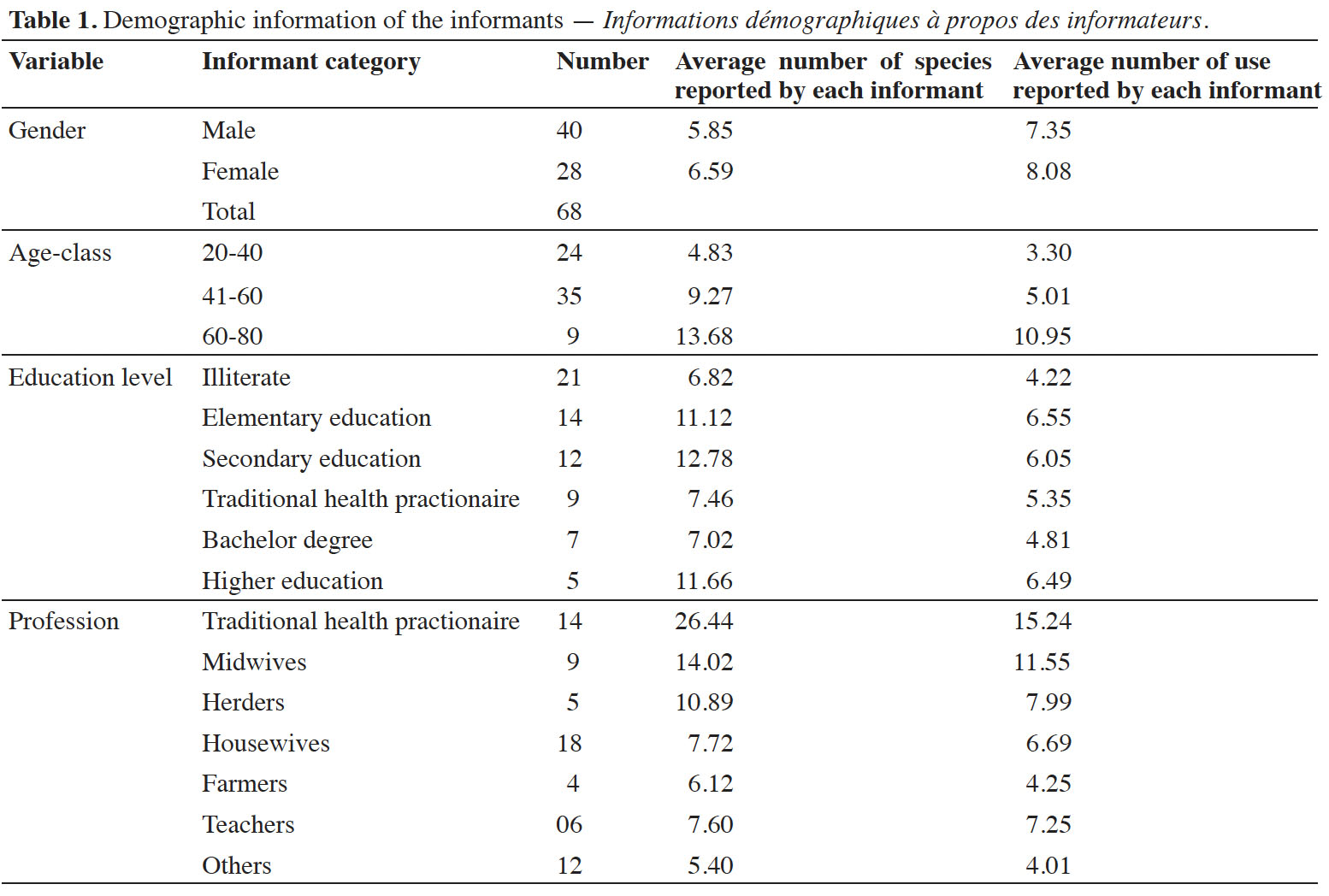
25The ethnopharmacological data were gained from 68 participants during field visits. Information on age, gender, education and profession of the participants was documented. Of the participants 58% were men and 41% women (Table 1). Older participants (age ≥ 60) held wider traditional knowledge regarding preparation and administration of ethnomedicines (average known species = 13.68; average known uses = 10.95) followed by middle aged people (age = 40-60), as compared to younger informants (age = 19-40).
3.2. Ethno-floral diversity
26A total of 140 medicinal plant species belonging to 54 families and 123 genera were recorded. In the study area herbaceous species were prevalent with a contribution of 72.85%, followed by shrubs (13.57%) and trees (13.57%). Asteraceae (14 species) and Rosaceae (13) were the most species rich medicinal plant families in the area (Figure 3).
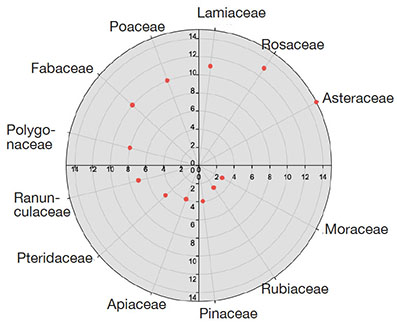
Figure 3. Family contribution of medicinal flora in the study area — Contribution de la famille de la flore médicinale dans la zone d’étude.
3.3. Plant parts used
27Various plant parts were used in preparation of different herbal remedies. Leaves (74 species) were most commonly used, followed by roots (46 species) and whole plant (34) (Figure 4).
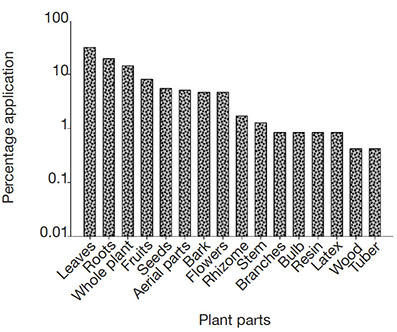
Figure 4. Plant parts used in herbal recipes — Parties de plantes utilisées dans les recettes à base de plantes.
3.4. Methods of preparation and mode of administration
28Different modes of preparation were used by local inhabitants for the preparation of herbal remedies. Decoction was the most important method of herbal preparation (45 species) followed by paste (37 species), juice and extract (29 species each).
3.5. Relative frequency citation (RFC) and use value (UV)
29The relative frequency citation is used to determine commonly occurring medicinal plants used to treat different ailments by the local inhabitants. The relative frequency of citation in the current study ranged between 0.02-0.89. The important medicinal plant species with highest RFC values were Thymus linearis Benth. (0.89) and Geranium wallichianum D.Don ex Sweet (0.89). They were followed by Berberis lycium Royle (0.88), Elaeagnus umbellata Thunb. (0.88), Bergenia ciliata (Haw.) Sternb. (0.88), Cynodon dactylon (L.) Pers. (0.86), Viola canescens Wall., Eriocapitella rupicola (0.85) and Mentha longifolia (L.) L. (0.80) (Annex 1).
3.6. Relative Importance (RI)
30The highest relative importance values were found for Allium cepa L. (100), Oxalis corniculata L., Alcea rosea (L.) Cav. (92.5 each), Rosa brunonii Lindl. (85.5), Agrimonia eupatoria L. (72.5 each), G. wallichianum, Allium sativum L., Anaphalis margaritacea (L.) Benth. & Hook.f. (81 each) and Plantago lanceolata L., Origanum vulgare L. (79.5 each) (Annex 1), showing local peoples’ familiarity about these plants.
3.7. Informant Consensus Factor (ICF)
31The local inhabitants of the area used plants for curing a wide variety of diseases. The diseases were broadly classified into 16 categories. Data was arranged on the basis of local classification system developed by traditional healers. The ICF values range from 0.66-0.92. The highest ICF value was recorded for circulatory disorders (0.92), followed by digestive disorders (0.91) and skin aliments (0.86) (Figure 5). The most commonly used plants were R. brunonii, B. lycium, A. rosea, M. longifolia, Quercus robur L., Aesculus indica (Wall. ex Cambess.) Hook., Pyrus pashia Buch.-Ham. ex D.Don, Vachellia nilotica (L.) P.J.H. Hurter & Mabb., Melia azedarach L., Pinus roxburghii Sarg., Punica granatum L., Pinus wallichiana A.B.Jacks., Cedrus deodara (Roxb. ex D.Don) G.Don, Abies pindrow (Royle ex D.Don) Royle, Ficus palmata Forssk., Sarcococca saligna Müll.Arg., Rubus niveus Wall. and Salix nigra Marshall.
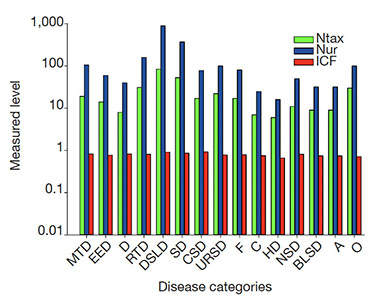 Figure 5. Informant consensus factor of diseases with use reports and total number of species used — Facteur de consensus des informateurs sur les maladies avec rapports d’utilisation et nombre total d’espèces utilisées.
Figure 5. Informant consensus factor of diseases with use reports and total number of species used — Facteur de consensus des informateurs sur les maladies avec rapports d’utilisation et nombre total d’espèces utilisées.
Ntax: total species used by all the informants for group of ailments — total des espèces utilisées par tous les informateurs pour le groupe de maladies; Nur: total number of use reports in each group of disease — nombre total de rapports d’utilisation dans chaque groupe de maladie; ICF: informant consensus factor — facteur de consensus des informateurs; MTD: mouth-throat — bouche-gorge; EED: eye and ear diseases — maladies des yeux et des oreilles; D: diabetes — diabètes; RTD: respiratory diseases — maladies respiratoires; DSLD: digestive system and liver diseases — maladies du système digestif et du foie; SD: skin diseases — maladies de la peau; CSD: circulatory system diseases — maladies du système circulatoire; URSD: urinary and reproductive system diseases — maladies du système urinaire et reproductif; F: fever — fièvre; C: cancer — cancer; HP: hair problem — problème de cheveux; NSD: nervous system disorder — désordre du système nerveux; BLSD: blood and lymphatic system diseases — maladies du système sanguin et lymphatique; A: antidotes — antidotes; O: others — autres.
3.8. Fidelity level (FL)
32The fidelity level of the 63 most important plant species reported by the respondents for the treatment of specific diseases ranged between 13.6 to 100% (Annex 2). Berberis lycium, Zanthoxylum alatum Roxb., E. umbellata, V. canescens, M. longifolia, Bistorta amplexicaulis (D.Don) Greene and T. linearis showed 100% FL (Figure 6). These species were mostly used to treat wounds, gas, diabetes, flu, and backache. The other plant species with high FL included G. wallichianum (93.3%) to strengthen bones, P. wallichiana (91%) used to treat wounds, Acacia nilotica (L.) Delile (87.5%) to treat diarrhea, Micromeria biflora (Buch.-Ham. ex D.Don) Benth. (87.1%) used as against constipation, Cynodon dactylon (L.) Pers. (84.8%) to treat damaged bones, Rumex dentatus L. (84.6%) to treat joint pain, Ajuga bracteosa Wall. ex Benth. (79.4%) for blood circulation, Euphorbia wallichii Hook.f. (76.4 %) to treat dyspepsia, Achillea millefolium L. (76.1%) to treat tongue infection.
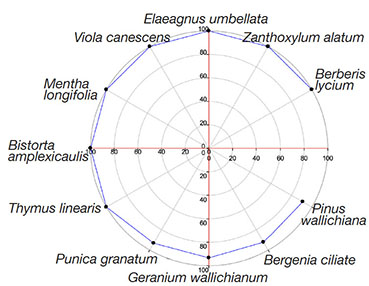 Figure 6. Top ranked plant species with above 80% fidelity — Les espèces végétales les mieux classées avec une fidélité supérieure à 80 %.
Figure 6. Top ranked plant species with above 80% fidelity — Les espèces végétales les mieux classées avec une fidélité supérieure à 80 %.
3.9. Jaccard Index (JI)
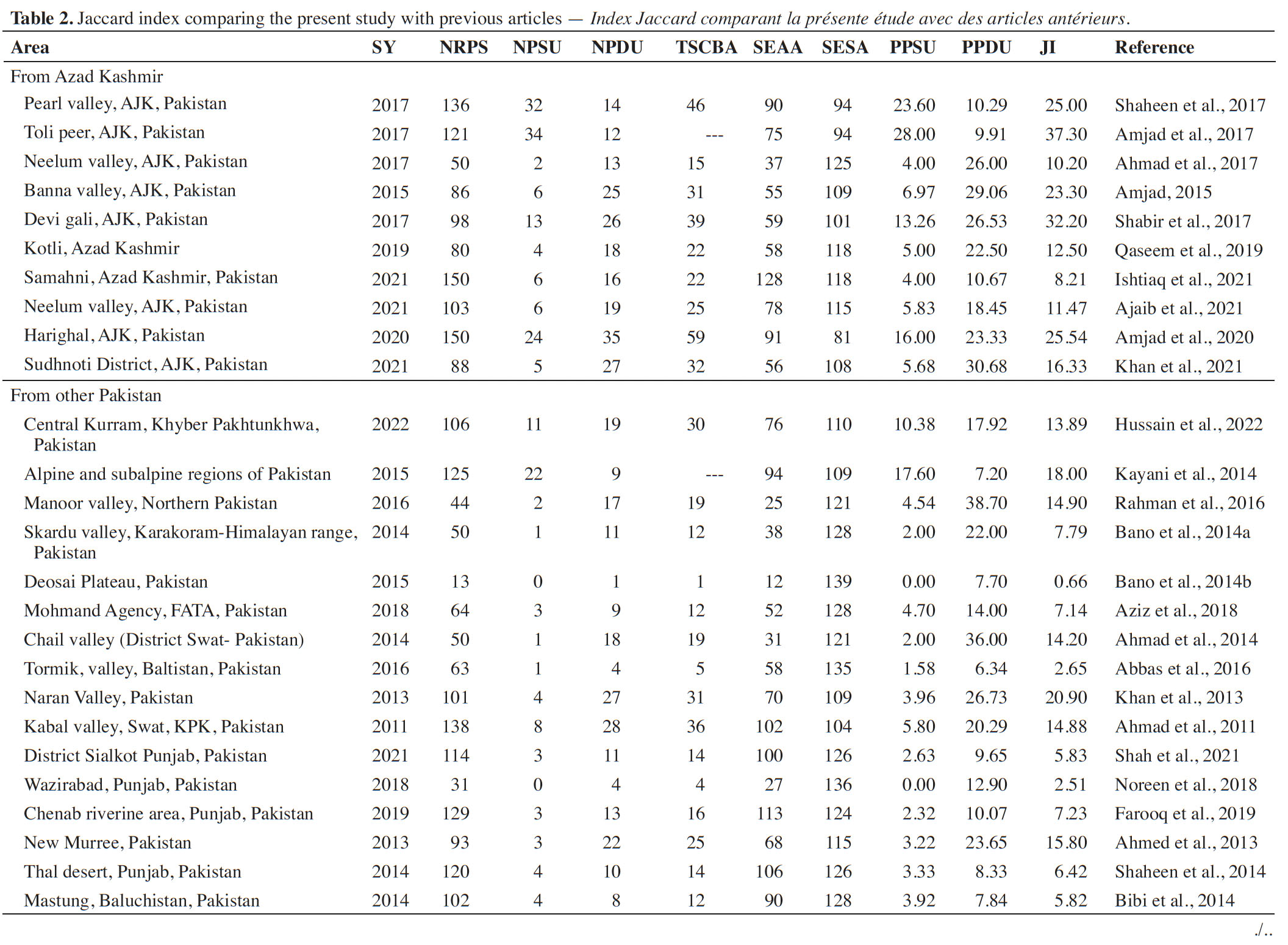
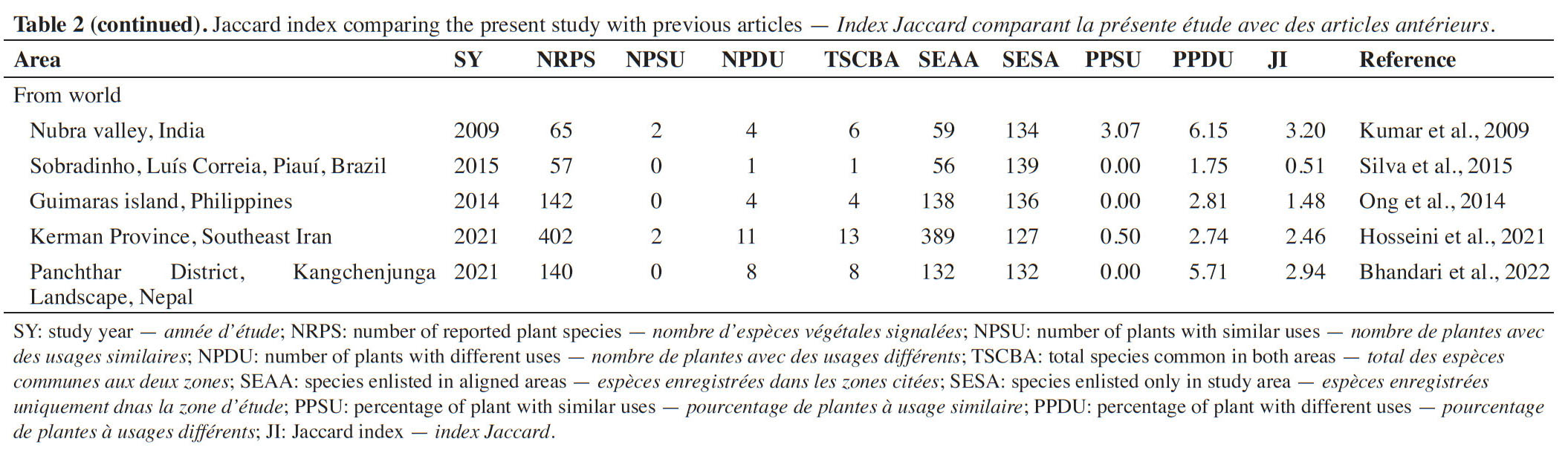
33Ethnomedicinal knowledge reported in the current study was compared with previous published ethnobotanical studies from communities at regional and international level (Table 2).
4. Discussion
4.1. Demographic data
34The majority of informants were men, as due to cultural restrictions they were much more easily approachable for data collection. Women however had significantly higher knowledge about medicinal plants (average number of species = 6.59; average number of uses = 8.08) compared to male informants. The reason for this may lie in their close association with the domestic life. Women generally use herbal preparation to keep their family healthy. Some other studies conducted in Pakistan and abroad also reported similar trends (Albuquerque et al., 2011; Ahmad et al., 2014; Kayani et al., 2014; Shaheen et al., 2017; Umair et al., 2019). Older people had much experience, skill and awareness regarding the preparation and administration of herbal remedies. This trend is very common in literature (Butt et al., 2015; Ahmad et al., 2017; Farooq et al., 2019). Education was inversely linked to ethnomedicinal knowledge, given that many educated people lack interest to learn and practice folk uses of medicinal plants. Our results are strongly supported by other studies (Giday et al., 2009; Tugume et al., 2010; Farooq et al., 2019). Traditional health practitioners (THP’s) and midwives held especially significant knowledge about medicinal plants. The trend of knowledge loss among younger generations is due to modern health facilities and changing life style. Similar trends were also observed in previous studies (Ahmad et al., 2017; Amjad et al., 2017; Farooq et al., 2019).
4.2. Ethno-floral diversity
35The research area is mountainous, with a high moisture level year-round, leading to the dominance of herbaceous species, similar to many regions throughout the world (Ahmad et al., 2014; Kayani et al., 2014; Shaheen et al., 2017). Asteraceae and Rosaceae were the most species rich medicinal plant families in the area. Many other studies also reported the dominance of Asteraceae (Bano et al., 2014b; Blanco et al., 1999; Tugume et al., 2010) and Rosaceae (Ahmad et al., 2014; Kayani et al., 2014). The reason for this might be the presence of a high proportion of bioactive components among the majority of the members of these families, with strong pharmacological and organoleptic properties. Similarly, findings were also reported by other researchers (Pieroni, 2008; Menković et al., 2011; Qaseem et al., 2019).
4.3. Plant parts used
36The widespread utilization of leaves in herbal remedies is explained by the richness of metabolites in leaves. Another reason is that leaves, in comparison to other plant parts, are abundant in nature and are easily available. Leaves were also the most used plant part in other studies (Cornara et al., 2009). Root was the second most commonly used plant part in the preparation of herbal recipes. It has been shown that roots often contain high concentrations of bioactive compounds as compared to other plant parts (Basualdo et al., 1995). In case of herbaceous species, the whole plants were frequently used. The removal of whole plant or roots or excessive use of fruits or seeds as medicines might however cause a decline in the plant populations, and therefore leaves are often more extensively used in herbal preparations (Giday et al., 2003; Ghimire et al., 2008).
4.4. Methods of preparation and mode of administration
37The wide use of decoction coincided with many previous studies (Qaseem et al., 2019). The frequent use of decoction might be due to the effectiveness of heat for many active compounds (Zhang et al., 2005; Han et al., 2007; Chen et al., 2008). Decoctions can be prepared easily by mixing with water, tea and soup. Sometimes honey and sugar may also be added (Harmayani et al., 2019).
4.5. Quantitative ethnobotanical indices
38Use value (UV). Use value is the measure of use types that were related to a particular plant species. A high use value reveals the importance of a species for treating different disorders. High use value also indicates that a plant species is well known and frequently used by the studied population (Kayani et al., 2014). Many of these plant species were abundant in the study area, and local inhabitants were well familiar with them. The plants with high use value are expected to be biologically more active (Trotter et al., 1986). The plants with highest RFC values should be used in phytochemical and pharmacological studies to assess their validity for possible drug development (Mukherjee et al., 2012).
39Informant Consensus Factor (ICF). The maximum ICF value was reported for gastro-intestinal and parasitic disorders. Gastro-intestinal diseases were widespread in the area which can be attributed to inadequate accessibility of clean food and drinking water. Similar results for gastro-intestinal disorders were also reported by other studies (Murad et al., 2013; Malla et al., 2015; Tangjitman et al., 2015). Skin disorders were also common among the inhabitants leading to high ICF value (Shaheen et al., 2017; Farooq et al., 2019).
40Fidelity level (FL). Berberis lycium, Z. alatum, E. umbellata, V. canescens, M. longifolia, B. amplexicaulis and T. linearis showed 100% FL. High FL indicates abundant utilization of a plant species to treat a specific disease in an area (Srithi et al., 2009; Bibi et al., 2014). Plants with high FL value have potential to be used in advanced ethnopharmacological research (Hassan-Abdallah et al., 2013).
41Jaccard Index (JI). Differences in ecological (Ladio et al., 2007), historical (Moerman, 1989), organoleptic and phytochemical factors have been elucidated as being responsible for variance and resemblance of indigenous knowledge among communities. Comparisons of communities can be giving valuable leads for the development of new drugs (Leonti et al., 2009). The data shows that the similarity percentage of uses ranged between 0% to 28% and the dissimilarity from 1.75% to 38.7%. The maximum level of similarity was found with communities studied in Toli peer (Amjad et al., 2017) and Pearl valley (Shaheen et al., 2017) with JI values of 37.3 and 25 respectively. The distances between the study area and allied communities are seen as mostly responsible for differences in the value of the JI. The communities closer to the study area had a high similarity index value. This can also be related to similar vegetation and high cultural exchange in the past between the local communities, resulting in the similarity in the ethnobotanical knowledge of allied areas.
42The lowest value of similarity indices was recorded for the studies conducted in Sobradinho, Luís Correia, Piauí, Brazil (Silva et al., 2015) and Guimaras Island (Ong et al., 2014), which, given the completely different flora and cultural background, is not surprising. The comparative analysis of our research with published studies highlighted some novel uses of plants not reported so far from the region including the use of a leaf decoction of Hepatica falconeri (Thomson) Yuz. for diabetes, the whole plant pastes of Clinopodium umbrosum (M.Bieb.) Kuntze for wounds healing, a whole plant extract of Anisomeles indica (L.) Kuntze used as blood purifier, aerial parts of Galium aparine L. used to stop bleeding, and the fruits of Daphne papyracea Wall. ex G. Don eaten for tonsilitis. The plant species with novel medicinal uses and high RFC value should be studied to elucidate bioactive compounds and pharmacological activities for the possible development of novel drugs.
5. Conclusions
43The current study is the first documentation of indigenous knowledge about the medicinal flora of Lasdana. Quantitative indices including relative frequencies of citation (RFC), use value (UV), fidelity level (FL), relative importance (RI), informant consensus factor (ICF) and Jaccard index (JI) confirmed that the area is rich in botanical and cultural diversity. The population of the area largely depends upon wild plants for primary health care. However, traditional knowledge is gradually decreasing in the new generation. This study provides baseline information for the conservation and sustainable use of the local flora.
Acknowledgements
44We are thankfull to people of Lasdana, Azad Jammu & Kashmir who share their valuable information during the study.
Bibliographie
Abbas Z. et al., 2016. Ethnobotany of the Balti community, Tormik valley, Karakorum range, Baltistan, Pakistan. J. Ethnobiol. Ethnomed., 12, 38, doi.org/10.1186/s13002-016-0114-y
Adnan M. et al., 2014. Ethnomedicine use in the war affected region of northwest Pakistan. J. Ethnobiol. Ethnomed., 10, 16, doi.org/10.1186/1746-4269-10-16
Ahmad I., Ibrar M. & Ali N., 2011. Ethnobotanical study of Tehsil Kabal, Swat District, KPK, Pakistan. J. Bot., article ID 368572, doi.org/10.1155/2011/368572
Ahmad K.S. et al., 2017. Ethnopharmacological studies of indigenous plants in Kel village, Neelum Valley, Azad Kashmir, Pakistan. J. Ethnobiol. Ethnomed., 13, 1-8, doi.org/10.1186/s13002-017-0196-1
Ahmad M. et al., 2014. An ethnobotanical study of medicinal plants in high mountainous region of Chail valley (District Swat-Pakistan). J. Ethnobiol. Ethnomed., 10, 36, doi.org/10.1186/1746-4269-10-36
Ahmed E. et al., 2013. Ethnobotanical appraisal and medicinal use of plants in Patriata, New Murree, evidence from Pakistan. J. Ethnobiol. Ethnomed., 9, 13, doi.org/10.1186/1746-4269-9-13
Ajaib M. et al., 2021. Inventorization of traditional ethnobotanical uses of wild plants of Dawarian and Ratti Gali areas of District Neelum, Azad Jammu and Kashmir Pakistan. Plos one, 16, p.e0255010, doi.org/10.1371/journal.pone.0255010
Albuquerque U.P.D. et al., 2011. The use of plants in the medical system of the Fulni-ô people (NE Brazil): a perspective on age and gender. J. Ethnopharmacol., 133, 866-873, doi.org/10.1016/j.jep.2010.11.021
Alexiades M.N. & Sheldon J.W., 1996. Selected guidelines for ethnobotanical research: a field manual. Boranx, NY, USA: The New York Botanical Garden.
Amjad M.S., 2015. Ethnobotanical profiling and floristic diversity of Bana Valley, Kotli (Azad Jammu and Kashmir), Pakistan. Asian Pac. J. Trop. Biomed., 5, 292-299, doi.org/10.1016/s2221-1691(15)30348-8
Amjad M.S. et al., 2017. Descriptive study of plant resources in the context of the ethnomedicinal relevance of indigenous flora: a case study from Toli Peer National Park, Azad Jammu and Kashmir, Pakistan. PloS one, 12, e0171896, doi.org/10.1371/journal.pone.0171896
Amjad M.S. et al., 2020. Ethnobotanical survey of the medicinal flora of Harighal, Azad Jammu & Kashmir, Pakistan. J. Ethnobiol. Ethnomed., 16, 1-28, doi.org/10.1186/s13002-020-00417-w
Anam S. et al., 2017. Ethno botanical wisdom of inhabitant of Devi Galli Azad Kashmir. Biomed. J. Sci. Tech. Res., 1(6), doi.org/10.26717/BJSTR.2017.01.000501
Aziz M.A. et al., 2018. Traditional uses of medicinal plants practiced by the indigenous communities at Mohmand Agency, FATA, Pakistan. J. Ethnobiol. Ethnomed., 14, 1, doi.org/10.1186/s13002-017-0204-5
Bano A. et al., 2014a. Quantitative ethnomedicinal study of plants used in the Skardu valley at high altitude of Karakoram-Himalayan range, Pakistan. J. Ethnobiol. Ethnomed., 10, 43-71, doi.org/10.1186/1746-4269-10-43
Bano A. et al., 2014b. Ethnomedicinal knowledge of the most commonly used plants from Deosai Plateau, Western Himalayas, Gilgit Baltistan, Pakistan. J. Ethnopharmacol., 155, 1046-1052, doi.org/10.1016/j.jep.2014.05.045
Basualdo I., Zardini E.M. & Ortiz M., 1995. Medicinal plants of Paraguay: underground organs, II. Econ. Bot., 49, 387-394, doi.org/10.1007/bf02863089
Baydoun S., Chalak L., Dalleh H. & Arnold N., 2015. Ethnopharmacological survey of medicinal plants used in traditional medicine by the communities of Mount Hermon, Lebanon. J. Ethnopharmacol., 173, 139-156, doi.org/10.1016/j.jep.2015.06.052
Bhandari P. et al., 2021. Traditional use of medicinal plants in the Chyangthapu-Phalaicha biological sub-corridor, Panchthar District, Kangchenjunga Landscape, Nepal. Ethnobot. Res. Appl., 22, 1-43, doi.org/10.32859/era.22.25.1-43
Bibi T. et al., 2014. Ethnobotany medicinal plants in district Mastung of Balochistan province-Pakistan. J. Ethnopharmacol., 157, 79-89, doi.org/10.1016/j.jep.2014.08.042
Blanco E., Macıa M. & Morales R., 1999. Medicinal and veterinary plants of El Caurel (Galicia, northwest Spain). J. Ethnopharmacol., 65, 113-124, doi.org/10.1016/s0378-8741(98)00178-0
Bruni A., Ballero M. & Poli F., 1997. Quantitative ethnopharmacological study of the Campidano Valley and Urzulei district, Sardinia, Italy. J. Ethnopharmacol., 57, 97-124, doi.org/10.1016/s0378-8741(97)00055-x
Butt M.A. et al., 2015. Ethnomedicinal uses of plants for the treatment of snake and scorpion bite in Northern Pakistan. J. Ethnopharmacol., 168, 164-181, doi.org/10.1016/j.jep.2015.03.045
Chase M.W. et al., 2016. An update of the Angiosperm Phylogeny Group classification for the orders and families of flowering plants: APG IV. Bot. J. Linn. Soc., 181, 1-20, doi.org/10.1111/boj.12385
Chen G. et al., 2008. Comparative analysis on microbial and rat metabolism of ginsenoside Rb1 by high‐performance liquid chromatography coupled with tandem mass spectrometry. Biomed. Chromatogr., 22, 779-785, doi.org/10.1002/bmc.1001
Cornara L., La Rocca A., Marsili S. & Mariotti M., 2009. Traditional uses of plants in the Eastern Riviera (Liguria, Italy). J. Ethnopharmacol., 125, 16-30, doi.org/10.1016/j.jep.2009.06.021
Edwards S., Nebel S. & Heinrich M., 2005. Questionnaire surveys: methodological and epistemological problems for field-based ethnopharmacologists. J. Ethnopharmacol., 100, 30-36, doi.org/10.1016/j.jep.2005.05.026
Farooq A. et al., 2019. Ethnomedicinal knowledge of the rural communities of Dhirkot, Azad Jammu and Kashmir, Pakistan. J. Ethnobiol. Ethnomed., 15, 1-30, doi.org/10.1186/s13002-019-0323-2
Ghimire S.K. et al., 2008. Demographic variation and population viability in a threatened Himalayan medicinal and aromatic herb Nardostachys grandiflora: matrix modelling of harvesting effects in two contrasting habitats. J. Appl. Ecol., 45, 41-51, doi.org/10.1111/j.1365-2664.2007.01375.x
Ghorbani A., Langenberger G., Feng L. & Sauerborn J., 2011. Ethnobotanical study of medicinal plants utilised by Hani ethnicity in Naban river watershed national nature reserve, Yunnan, China. J. Ethnopharmacol., 134, 651-667, doi.org/10.1016/j.jep.2011.01.011
Giday M., Asfaw Z., Elmqvist T. & Woldu Z., 2003. An ethnobotanical study of medicinal plants used by the Zay people in Ethiopia. J. Ethnopharmacol., 85, 43-52, doi.org/10.1016/s0378-8741(02)00359-8
Giday M., Asfaw Z. & Woldu Z., 2009. Medicinal plants of the Meinit ethnic group of Ethiopia: an ethnobotanical study. J. Ethnopharmacol., 124, 513-521, doi.org/10.1016/j.jep.2009.05.009
Gonza T.M. et al., 2008. Medicinal plants in the Mediterranean area: synthesis of the results of the project RUBIA. J. Ethnopharmacol., 116, 341-357, doi.org/10.1016/j.jep.2007.11.045
Han J. et al., 2007. Analysis of multiple constituents in a Chinese herbal preparation Shuang-Huang-Lian oral liquid by HPLC-DAD-ESI-MSn. J. Pharm. Biomed. Anal., 44, 430-438, doi.org/10.1016/j.jpba.2007.02.023
Harmayani et al., 2019. Healthy food traditions of Asia: exploratory case studies from Indonesia, Thailand, Malaysia, and Nepal. J. Ethnic Foods, 6, doi.org/10.1186/s42779-019-0002-x
Hassan-Abdallah A. et al., 2013. Medicinal plants and their uses by the people in the region of Randa, Djibouti. J. Ethnopharmacol., 148, 701-713, doi.org/10.1016/j.jep.2013.05.033
Heinrich M., 2008. Ethnopharmacy and natural product research—Multidisciplinary opportunities for research in the metabolomic age. Phytochem. Lett., 1, 1-5, doi.org/10.1016/j.phytol.2007.11.003
Heinrich M. et al., 1998. Medicinal plants in Mexico: healers' consensus and cultural importance. Soc. Sci. Med., 47, 1859-1871, doi.org/10.1016/j.jep.2013.05.033
Heinrich M., Edwards S., Moerman D.E. & Leonti M., 2009. Ethnopharmacological field studies: a critical assessment of their conceptual basis and methods. J. Ethnopharmacol., 124, 1-17, doi.org/10.1016/j.jep.2009.03.043
Hosseini S.H. et al., 2021. Ethnobotany of the medicinal plants used by the ethnic communities of Kerman province, Southeast Iran. J. Ethnobiol. Ethnomed., 17, 1-35, doi.org/10.1186/s13002-021-00438-z
Hussain S. et al., 2022. Quantitative ethnomedicinal study of indigenous knowledge on medicinal plants used by the tribal communities of Central Kurram, Khyber Pakhtunkhwa, Pakistan. Ethnobot. Res. Appl., 23, 1-31, doi.org/10.32859/era.23.5.1-31
Ishtiaq M. et al., 2021. Ethnomedicinal and folklore inventory of wild plants used by rural communities of valley Samahni, District Bhimber Azad Jammu and Kashmir, Pakistan. Plos one, 16, p.e0243151, doi.org/10.1371/journal.pone.0243151
Kadam P. & Bhalerao S., 2010. Sample size calculation. Int. J. Ayurveda Res., 1, 55.
Kayani S. et al., 2014. Ethnobotanical uses of medicinal plants for respiratory disorders among the inhabitants of Gallies–Abbottabad, Northern Pakistan. J. Ethnopharmacol., 156, 47-60, doi.org/10.1016/j.jep.2014.08.005
Khan M.F. et al., 2021. An ethnopharmacological survey and comparative analysis of plants from the Sudhnoti District, Azad Jammu and Kashmir, Pakistan. J. Ethnobiol. Ethnomed., 17, 1-22, doi.org/10.1186/s13002-021-00435-2
Khan M.P.Z. et al., 2015. Ethnomedicinal uses of edible wild fruits (EWFs) in Swat Valley, Northern Pakistan. J. Ethnopharmacol., 173, 191-203, doi.org/10.1016/j.jep.2015.07.029
Khan S.M. et al., 2013. Medicinal flora and ethnoecological knowledge in the Naran Valley, Western Himalaya, Pakistan. J. Ethnobiol. Ethnomed., 9(4), doi.org/10.1186/1746-4269-9-4
Kumar G., Gupta S., Murugan M. & Singh B.S., 2009. Ethnobotanical studies of Nubra Valley-A cold arid zone of Himalaya. Ethnobot. Leafl., 6, 9.
Ladio A., Lozada M. & Weigandt M., 2007. Comparison of traditional wild plant knowledge between aboriginal communities inhabiting arid and forest environments in Patagonia, Argentina. J. Arid Environ., 69, 695-715, doi.org/10.1016/j.jaridenv.2006.11.008
Leonti M., Casu L., Sanna F. & Bonsignore L., 2009. A comparison of medicinal plant use in Sardinia and Sicily—De materia medica revisited. J. Ethnopharmacol., 121, 255-267, doi.org/10.1016/j.jep.2008.10.027
Malla B., Gauchan D.P. & Chhetri R.B., 2015. An ethnobotanical study of medicinal plants used by ethnic people in Parbat district of western Nepal. J. Ethnopharmacol., 165, 103-117, doi.org/10.1016/j.jep.2014.12.057
Menković N. et al., 2011. Ethnobotanical study on traditional uses of wild medicinal plants in Prokletije Mountains (Montenegro). J. Ethnopharmacol., 133, 97-107, doi.org/10.1016/j.jep.2010.09.008
Moerman D.E., 1989. Poisoned apples and honeysuckles: the medicinal plants of native America. Med. Anthropol. Q., 3, 52-61, doi.org/10.1525/maq.1989.3.1.02a00040
Mukherjee P.K., Nema N.K., Venkatesh P. & Debnath P.K., 2012. Changing scenario for promotion and development of Ayurveda way forward. J. Ethnopharmacol., 143, 424-434, doi.org/10.1016/j.jep.2012.07.036
Murad W. et al., 2013. Ethnobotanical assessment of plant resources of Banda Daud Shah, District Karak, Pakistan. J. Ethnobiol. Ethnomed., 9, 77, doi.org/10.1186/1746-4269-9-77
Nasir E., Ali S. & Stewart R.R., 1972. Flora of West Pakistan. In: Stewart R. An annotated catalogue of the vascular plants of West Pakistan and Kashmir. Karachi, Pakistan: Fakhri Printing Press.
Nasir Y.J. & Ali S., 2010. Flora of Pakistan. Karachi, Pakistan: Department of Botany, University of Karachi; Islamabad: National Herbarium.
Noreen F. et al., 2018. Data of ethnomedicinal plants in Wazirabad, District Gujranwala, Punjab, Pakistan. J. Pharm. Care Health Syst., 5, 1000194, doi.org/10.4172/2376-0419.1000194
Ong H.G. & Kim Y.D., 2014. Quantitative ethnobotanical study of the medicinal plants used by the Ati Negrito indigenous group in Guimaras island, Philippines. J. Ethnopharmacol., 157, 228-242, doi.org/10.1016/j.jep.2014.09.015
Pieroni A., 2008. Local plant resources in the ethnobotany of Theth, a village in the Northern Albanian Alps. Genet. Resour. Crop Evol., 55, 1197-1214, doi.org/10.1007/s10722-008-9320-3
Pieroni A. & Quave C.L., 2005. Traditional pharmacopoeias and medicines among Albanians and Italians in southern Italy: a comparison. J. Ethnopharmacol., 101, 258-270, doi.org/10.1016/j.jep.2005.04.028
Qaseem M.F. et al., 2019. Ethnobotanical evaluation of traditional medicinal plants among the rural communities of Goi and Dhanwa union council, District Kotli, Azad Jammu & Kashmir. Appl. Ecol. Environ. Res., 6, 340-349.
Rahman I.U. et al., 2016. Contributions to the phytotherapies of digestive disorders: traditional knowledge and cultural drivers of Manoor Valley, Northern Pakistan. J. Ethnopharmacol., 192, 30-52, doi.org/10.1016/j.jep.2016.06.049
Shabir A. et al., 2017. Ethno botanical wisdom of inhabitant of Devi Galli Azad Kashmir. Biomed. J. Sci. Techn. Res., 1, 1618-1627, doi.org/10.26717/bjstr.2017.01.000501
Shah S.A. et al., 2021. Ethnopharmacological study of medicinal plants in Bajwat Wildlife Sanctuary, District Sialkot, Punjab Province of Pakistan. Evid. Based Complementary Altern. Med., article ID 5547987, doi.org/10.1155/2021/5547987
Shaheen H., Qureshi R., Akram A. & Gulfraz M., 2014. Inventory of medicinal flora from Thal desert, Punjab, Pakistan. Afr. J. Tradit. Complementary Altern. Med., 11, 282-290, doi.org/10.4314/ajtcam.v11i3.39
Shaheen H., Qaseem M.F., Amjad M.S. & Bruschi P., 2017. Exploration of ethno-medicinal knowledge among rural communities of Pearl Valley; Rawalakot, District Poonch Azad Jammu and Kashmir. PloS one, 12, e0183956, doi.org/10.1371/journal.pone.0183956
Shinwari Z.K., 2010. Medicinal plants research in Pakistan. J. Med. Plant Res., 4, 161-176.
Silva J. et al., 2015. Ethnobotanical survey of medicinal plants used by the community of Sobradinho, Luís Correia, Piauí, Brazil. J. Med. Plant Res., 9(32), 872-883, doi.org/10.5897/jmpr2015.5881
Srithi K. et al., 2009. Medicinal plant knowledge and its erosion among the Mien (Yao) in northern Thailand. J. Ethnopharmacol., 123, 335-342, doi.org/10.1016/j.jep.2009.02.035
Tangjitman K. et al., 2015. Ethnomedicinal plants used for digestive system disorders by the Karen of northern Thailand. J. Ethnobiol. Ethnomed., 11, 27, doi.org/10.1186/s13002-015-0011-9
The Plant List, 2013. The plant list, version 1.1, http://www.theplantlist.org/, (31 March 2022).
Trotter R. & Logan M., 1986. Informant consensus: a new approach for identifying potentially effective medicinal plants. In: Etkin N.L. Plants and indigenous medicine and diet: biobehavioral approaches. Routledge.
Tugume P. et al., 2010. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J. Ethnobiol. Ethnomed., 12, 5, doi.org/10.1186/s13002-015-0077-4
Umair M., Altaf M., Bussmann R.W. & Abbasi A.M., 2019. Ethnomedicinal uses of the local flora in Chenab riverine area, Punjab province Pakistan. J. Ethnobiol. Ethnomed., 15(7), doi.org/10.1186/s13002-019-0285-4
Verpoorte R., Choi Y.H. & Kim H.K., 2005. Ethnopharmacology and systems biology: a perfect holistic match. J. Ethnopharmacol., 100, 53-56, doi.org/10.1016/j.jep.2005.05.033
Vijayakumar J. et al., 2015. Quantitative ethnomedicinal study of plants used in the Nelliyampathy hills of Kerala, India. J. Ethnopharmacol., 161, 238-254, doi.org/10.1016/j.jep.2014.12.006
Vitalini S. et al., 2013. Traditional knowledge on medicinal and food plants used in Val San Giacomo (Sondrio, Italy)—An alpine ethnobotanical study. J. Ethnopharmacol., 145, 517-529, doi.org/10.1016/j.jep.2012.11.024
Zhang J.l. et al., 2005. Chemical fingerprint and metabolic fingerprint analysis of Danshen injection by HPLC–UV and HPLC–MS methods. J. Pharm. Biomed. Anal., 36, 1029-1035, doi.org/10.1016/j.jpba.2004.09.009
